

Stony Coral Tissue Loss Disease (SCTLD) Case Definition for Wildlife
Links
- Document: Report (5.8 MB pdf) , HTML , XML
- Larger Work: Case definitions for wildlife diseases
- Download citation as: RIS | Dublin Core
Acknowledgments
We would like to thank the stony coral tissue loss disease histopathology subteam for the contribution of their time and collective expertise in the investigation and description of the microscopic characteristics of stony coral tissue loss disease.
Introduction
Diagnostic laboratories receive carcasses and samples for diagnostic evaluation and pathogen/toxin detection. The intent of a case definition is to provide scientifically based criteria for determining (1) if an individual carcass has a specific disease and the confidence of that diagnosis; and (2) if a pathogen or toxin is evident in a carcass or sample (for example, swab, tissue sample, skin scraping, blood/serum sample, environmental sample, or other). Using these criteria, cases diagnosed with a specific disease (diagnosing disease) will be classified as “confirmed,” “presumptive,” or “suspected;” and evidence of a pathogen or toxin (detecting pathogen/toxin) will be classified as “exposed” or “present/detected.” Classification is based on a combination of factors: individual, place, time, history, clinical signs, diagnostic observations, and (or) diagnostic test results. Case definitions bring clarity and consistency to the evaluation process. Their use within and between organizations allows more uniform reporting of diseases and etiologic agents.
Case definitions are proposed for use in wildlife diagnostic laboratories and are not intended to replace regulatory standards provided by Government reporting agencies. Ideally, case definitions would be updated periodically as new information becomes available and new test methods are developed. Refer to the glossary for terminology definitions.
Disease/condition.—Stony coral tissue loss disease (SCTLD)
Pathogen/toxin etiologic agent(s).—Unknown
Scope of the Case Definition
This case definition applies to several species of scleractinian corals across seven families: Family Faviidae (Gregory, 1900), including Colpophyllia natans (Houttuyn, 1772) (boulder brain coral), Diploria labyrinthiformis (Linnaeus, 1758) (grooved brain coral), Pseudodiploria clivosa (Ellis and Solander, 1786) (knobby brain coral), and P. strigosa (Dana, 1846) (symmetrical brain coral); Family Meandrinidae (Gray, 1847), including Dendrogyra cylindrus (Ehrenberg, 1834) (pillar coral), Dichocoenia stokesii (Milne-Edwards and Haime, 1848) (elliptical star coral), Eusmilia fastigiata (Pallas, 1766) (smooth flower coral), and Meandrina jacksoni (Weil and Pinzón, 2011) and M. meandrites (Linnaeus, 1758) (maze corals); Family Merulinidae (Verrill, 1866), including Orbicella franksi and O. annularis (Ellis and Solander, 1786) (boulder star corals), and O. faveolata (Ellis and Solander, 1786) (mountainous star coral); Family Montastraeidae, including Montastraea cavernosa (Linnaeus, 1767) (large-cup star coral); Family Astrocoeniidae (Koby, 1890), including Stephanocoenia intersepta (Lamarck, 1816) (blushing star coral); Family Scleractinia incertae sedis, including Solenastrea bournoni (Milne-Edwards and Haime, 1850) (smooth star coral); and Family Siderastreidae (Vaughan and Wells, 1943), including Siderastrea siderea (Ellis and Solander, 1786) (starlet coral) and possibly S. radians (Pallas, 1766) (starlet coral), although samples of this species were not collected (FDEP, 2018, Aeby and others, 2019).
Several other species are presumed susceptible, in Family Agariciidae (Gray, 1847), including Helioseris cucullata (Ellis and Solander, 1786) (sunray lettuce coral), Agaricia agaricites (Linnaeus, 1758), and other Agaricia spp. (Lamarck, 1801) (lettuce and plate/saucer corals); Family Faviidae, including Mycetophyllia spp. (Milne-Edwards and Haime, 1848) (cactus corals), Scolymia spp. (Haime, 1852) (disc corals), Isophyllia spp. (Milne-Edwards and Haime, 1851) (spinous cactus and rough star corals), and Mussa angulosa (Pallas, 1766) (spiny flower coral); and Family Pocilloporidae (Gray, 1842), including Madracis auretenra (pencil coral) (FDEP, 2018).
Of the tropical Western Atlantic scleractinian corals, members of the Family Poritidae (Gray, 1842), including Porites astreoides (Lamarck, 1816) (mustard hill coral), are considered to be of low susceptibility (Alvarez-Filip and others, 2019; Meiling and others, 2020, 2021); and members of the Family Oculinidae (Gray, 1847) have not been observed to be diseased during outbreaks. The acroporids Acropora palmata (Lamarck, 1816) (elkhorn coral) and A. cervicornis (Lamarck, 1816) (staghorn coral) are apparently not susceptible, nor are Cladocora spp. (Ehrenberg, 1834) (FDEP, 2018; Precht and others, 2016).
Case Definition Criteria
The case definition criteria are a concise summary of the current science regarding the clinical signs, history, gross and microscopic observations, and laboratory test results associated with a specific disease or pathogen. Various combinations of the criteria result in different case classifications representing the degree of certainty of the diagnosis.
Individual, Place, and Time Criteria for Diagnosis and Testing
Individual.—All ages and sizes of adult (sessile) coral are affected. Adult coral may be aged by annular rings in a manner like tree rings (Buddemeier, 1976). No data are available regarding larval stages. Larger colonies may survive longer and be therefore more likely to be observed, but larger size is not protective overall. Recently dead coral in an area experiencing an outbreak may be suspected as mortality caused by SCTLD (Aeby and others, 2019; Precht and others, 2016).
Place.—SCTLD has been documented along Florida’s Coral Reef (Florida Reef Tract) from Martin County south to Key West and now the Dry Tortugas (Muller and others, 2020; FDEP, 2018). Outbreaks of a disease with lesions grossly similar to SCTLD have also been confirmed in the Caribbean and Bahamas including Jamaica, Quintana Roo (Mexico), St. Maarten, St. Thomas, Dominican Republic, Turks and Caicos Islands, Saint-Martin, Belize, St. Eustatius, St. John, Puerto Rico, Grand Bahamas, Grand Cayman, United States and British Virgin Islands, Cayman Islands, Guadeloupe, and St. Lucia (Dahlgren, 2020; Marks and Lang, 2018). Honduras, Martinique, and Dominica were recently added to the Atlantic and Gulf Rapid Reef Assessment (AGRRA) dashboard (Kramer and others, 2019). Note that this disease is continuing to spread through the wider Caribbean and will almost certainly be present in new areas as time passes. Active surveillance of Pacific reefs is important because the Panama Canal could present a conduit for SCTLD into the Pacific, and susceptibility of Pacific species is unknown.
Time.—The SCTLD outbreak was noted in 2014 and was associated with unusually high temperatures, outflow of semi-treated sewage, and a dredging event in Miami harbor (Miller and others, 2016), and the disease has been consistently present in the Florida Reef Tract since that time. No clear pattern with respect to season has been identified (Aeby and others, 2019; Precht and others, 2016), but temperature increases have been associated with a decline in incidence and disease progression (Meiling and others, 2021; Williams and others, 2021).
Field Criteria for Diagnosis
History and clinical signs.—Diagnostically compatible illness may present with multifocal to coalescing sharply demarcated acute to subacute areas of tissue loss that may begin at the base of the colony and spread upwardly (apically) or appear randomly distributed. The area of tissue loss represented by bare skeleton may be bordered by a narrow band of bleached tissue but lacks any pigmented band at the tissue-loss margin. Skeleton at the tissue-loss margin is usually acute, appearing white and intact (depending upon species), although algae and fungal mats denoting older, subacute, or chronic lesions may accumulate on older areas of denuded skeleton.
Rapid rate of tissue loss, 5 to 40 square centimeters per day (Sharp and Maxwell, 2018), is highly suspicious but not pathognomonic for SCTLD (Bruckner, 2016). Affected individuals typically die within weeks to months depending on species (FDEP, 2018). The presence of multiple affected species on a reef consistent with the previously observed susceptible species also increases suspicion, as do proportionally large areas of tissue loss relative to colony size. Species that are more highly susceptible including boulder brain coral, pillar coral, elliptical star coral, grooved brain coral, maze coral, symmetrical brain coral, and knobby brain coral are typically affected first; and colonies may be discovered with complete mortality even on initial discovery. Species with intermediate susceptibility, including boulder star coral, mountainous star coral, large-cup star coral, smooth star coral, blushing star coral, and starlet coral show signs on average 1 month later and may die over months to years. Starlet coral is an exception and may show signs earlier, although progression may not match other species (FDEP 2018, Aeby and others 2019).
Other.—In Florida and aquaria experiments, induction of tissue loss appears to spread within the water column and through currents (Muller and others 2020), although natural water currents cannot explain spread throughout the Caribbean. Factors such as human activity and possible pathogen(s) transmission via contaminated bilge water and recreational or commercial equipment used in activities such as diving, boating, or fishing have all been suspected to play a role (Dahlgren, 2020). Because gross lesions alone are not diagnostic, SCTLD cannot be ruled in or out of a particular site distant from other affected areas if it meets current gross criteria of the case definition (refer to the “Laboratory Criteria for Diagnosis” section).
In laboratory studies, apparently healthy coral species exposed to affected wild corals by direct contact or indirect exposure developed the disease, so wild-collected coral are also a potential source of transmission (Aeby and others, 2019). However, to date no evidence of infectious agents consistently associated with SCTLD have been documented on light microscopy (Landsberg and others, 2020). Bacterial causes have been hypothesized, but no bacteria have been found consistently associated with lesions. Virus-like particles have been observed within endosymbionts of both SCTLD affected and apparently healthy exposed coral, causing lysis and death of affected endosymbionts, but more data are needed to conclusively tie these to disease (Work and others, 2021).
Laboratory Criteria for Diagnosis
Gross examination.—Diagnostically compatible findings may include focal or multifocal to coalescing patches of bleaching and tissue loss, or tissue loss beginning at the base of the colony that may be bordered by a narrow band of bleached tissue. For S. siderea, initial lesions may be purple or gray discolored tissue around the oral cavity rather than white denuded skeleton (fig. 1A). More chronic areas of denuded skeleton often develop a mat of fungal and (or) algal overgrowth, whereas areas of acute loss abut white, bare skeleton (Paul and others, 2019) (fig. 1B).
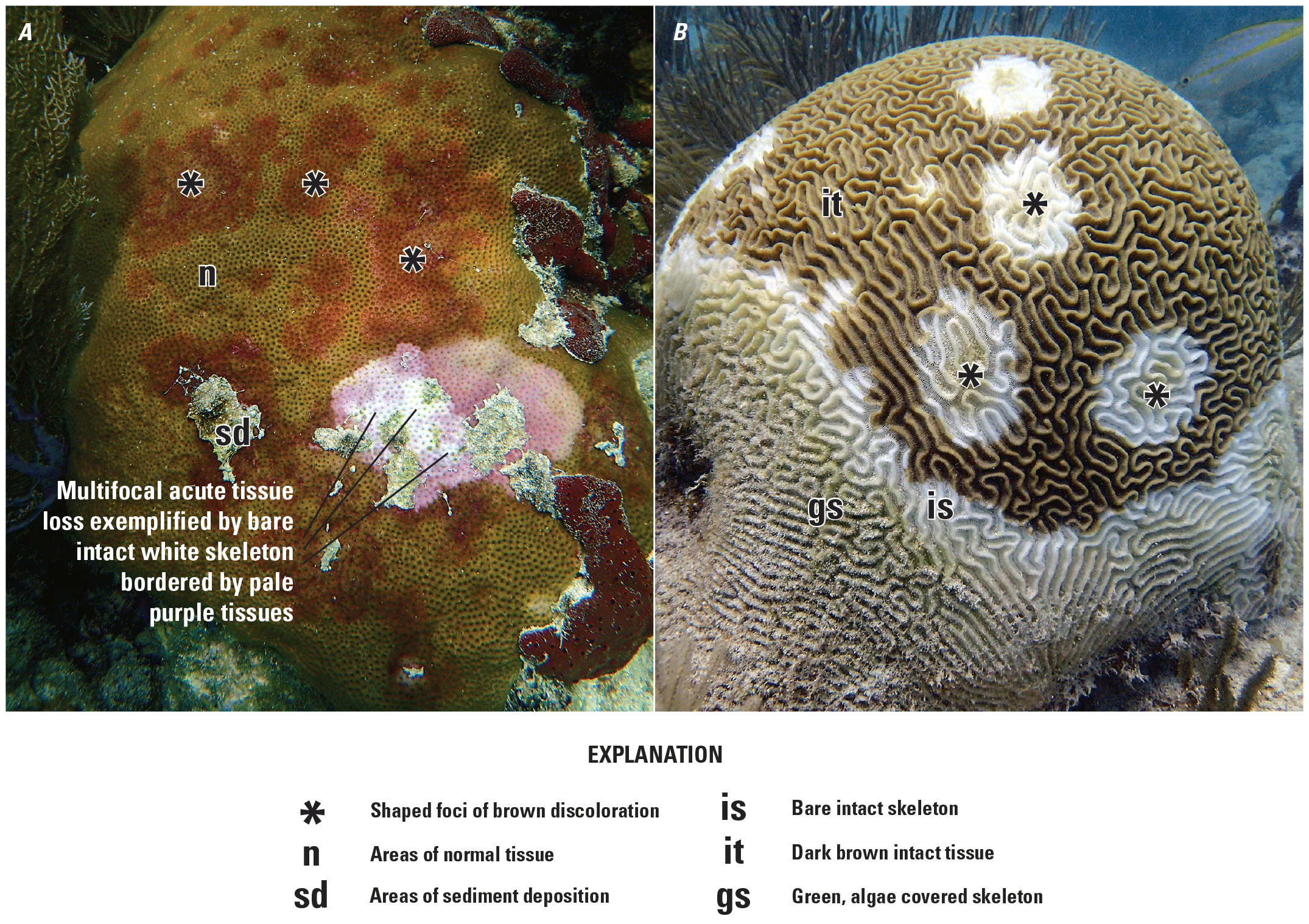
Gross appearance of stony coral tissue loss disease. Photographs by Andy Bruckner, Florida Keys National Marine Sanctuary. A, Siderastrea siderea (starlet coral) showing multifocal to coalescing, variably sized and shaped foci of brown discoloration sharply demarcated from the adjacent normal tissue, and multifocal acute tissue loss exemplified by bare intact white skeleton bordered by pale purple tissues and areas of sediment deposition. B, Colpophyllia natans (boulder brain coral) with multifocal and basal tissue loss exposing bare, white skeleton encroaching on the brown intact tissue. Note narrow band of bare denuded intact skeleton separating dark brown intact tissues from green skeleton with overgrowth by turf algae indicative of a subacute tissue loss process and older mortality (Work and Aeby, 2006).
Histopathology.—The histological presentation varies among species, and many affected species have not been examined microscopically. However, of those that have been examined (n=8), commonalities are described in this document and in (Landsberg and others, 2020). The tissue loss margin is often too autolyzed to be diagnostically useful, and apparently normal tissue on the affected colony distant from a lesion may be more diagnostic; therefore, biopsies should be taken from grossly normal areas of affected colonies as well as along the tissue loss margin. Histologic lesions can be seen in tissue far from the tissue loss margin in the coenenchyme or deeper in the polyp (fig. 2D).
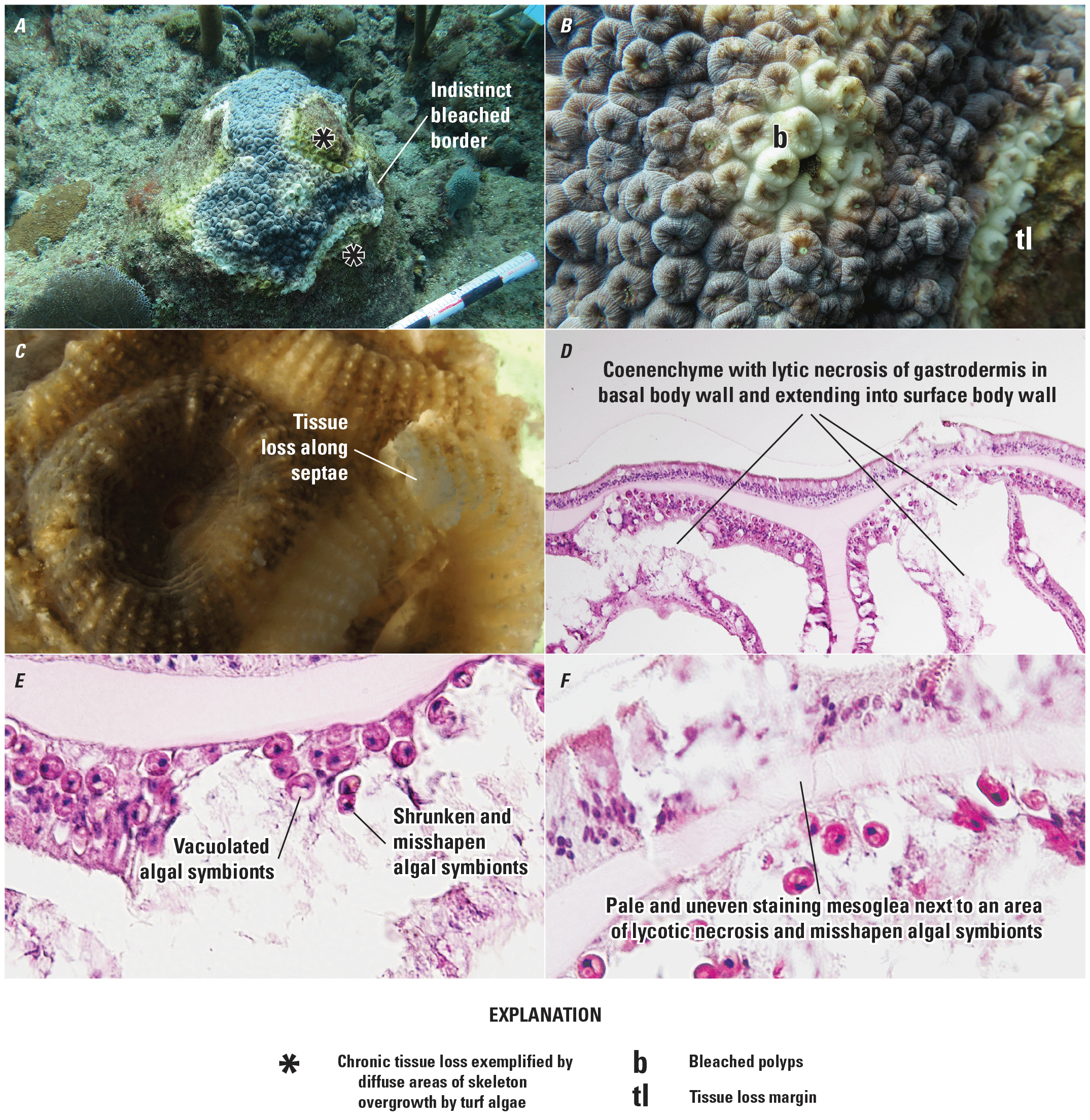
Montastraea cavernosa gross, subgross, and microscopic lesions. A, multifocal tissue loss; chronic tissue loss exemplified by diffuse areas of skeleton overgrowth by turf algae bordered by an indistinct bleached border and extending from the base of the colony. B, bleached polyps near tissue loss margin. Photograph by Vanessa Brinkhuis, Florida Fish and Wildlife Conservation Commission (FWC). C, subgross of affected polyps showing tissue loss along septae. Photograph by Yasu Kiryu, FWC. D, coenenchyme with lytic necrosis of gastrodermis in basal body wall and extending into surface body wall. E, shrunken, misshapen and vacuolated algal symbionts. F, pale, uneven staining mesoglea next to an area of lytic necrosis and misshapen algal symbionts. D, E, and F are paraffin embedded hematoxalin and eosin photomicrographs by Jan Landsberg and Yasu Kiru, FWC.
Histological lesions are first observed and most severe in the basal body wall of the gastrodermis and calicodermis, and center on the endosymbionts (Symbiodiniaceae) (figs. 3B, 3C). Endosymbionts show vacuolation, gray to brown discoloration and enlargement of the symbiosome (figs. 3D, 4D, 5D), or features of necrosis including deformation, cytoplasmic hypereosinophilia or hypopigmentation, swelling or shrinkage, nuclear pyknosis, karyorrhexis, or pallor with nuclear loss (ghost cells) (figs. 6D, 9D). In and around foci of affected algal symbionts, gastrodermis, especially at the basal body wall but also extending into the surface body wall, mesenteries, and cnidoglandular band, shows varying degrees of vacuolation attributed to increased mucocytes or cell swelling. There may also be characteristic discrete foci of lytic necrosis that have loss of cell detail (fig. 6B), disruption of tissue architecture, loss of endosymbionts, support cell necrosis, and detachment from the mesoglea (cleft formation) (figs. 7B, 8C). The mesoglea is often eroded (figs. 9C, 9D), pale, and displays irregular staining (fig. 8D, 9D). The calicodermis may be segmentally cuboidal to columnar (metaplastic) or sloughing and necrotic (figs. 8B, 8C).
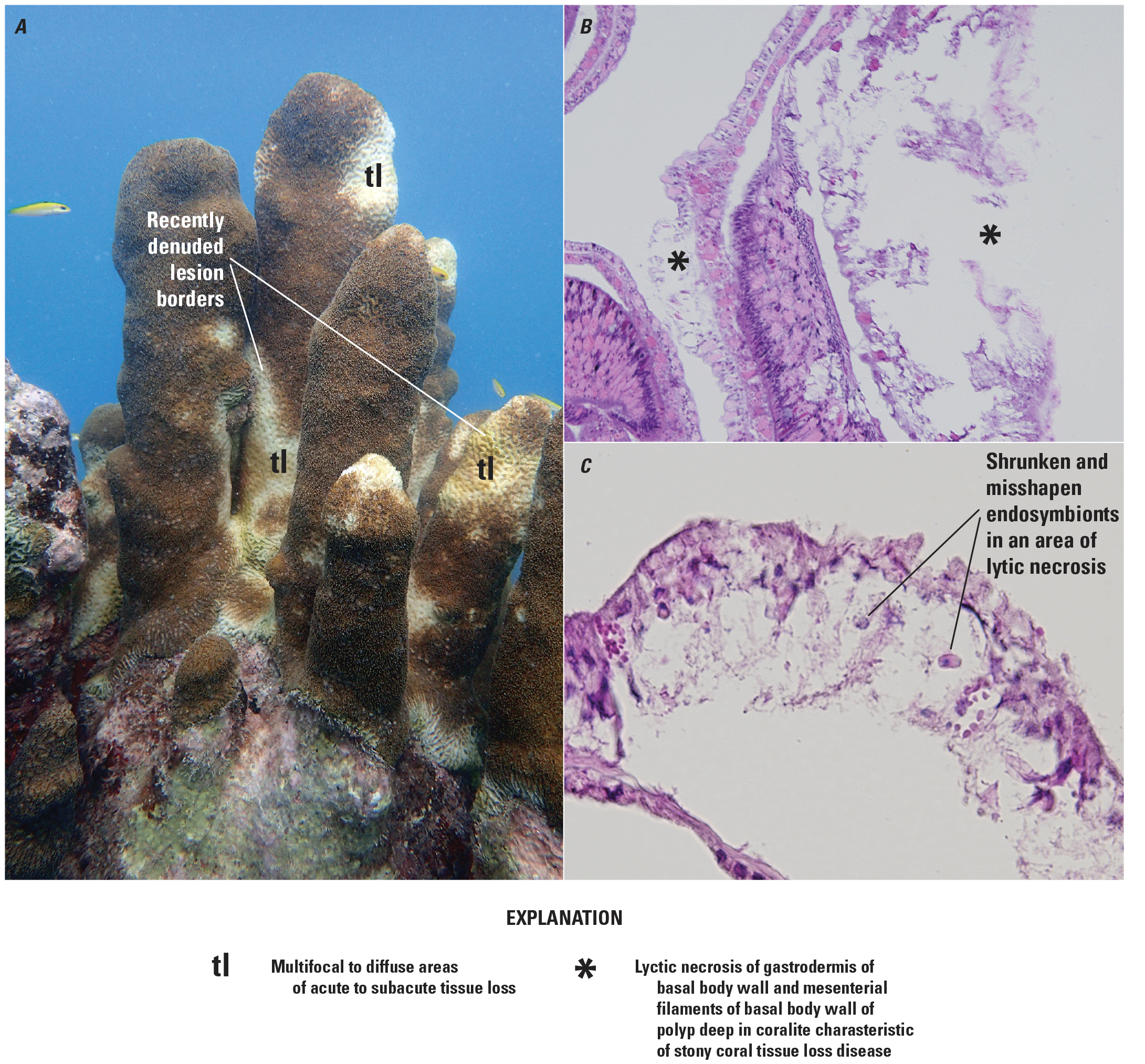
Dendrogyra cylindrus gross and microscopic lesions. A, multifocal to diffuse areas of acute to subacute tissue loss, some with narrow, white bleached indistinct, or recently denuded lesion borders. Photograph by Andy Bruckner, Florida Keys National Marine Sanctuary. B, lytic necrosis of gastrodermis of basal body wall and mesenterial filaments of basal body wall of polyp deep in corallite characteristic of stony coral tissue loss disease. C, shrunken, misshapen endosymbionts in area of lytic necrosis. B and C are paraffin embedded hematoxalin and eosin photomicrographs by Jan Landsberg and Yasu Kiryu, Florida Fish and Wildlife Conservation Commission.
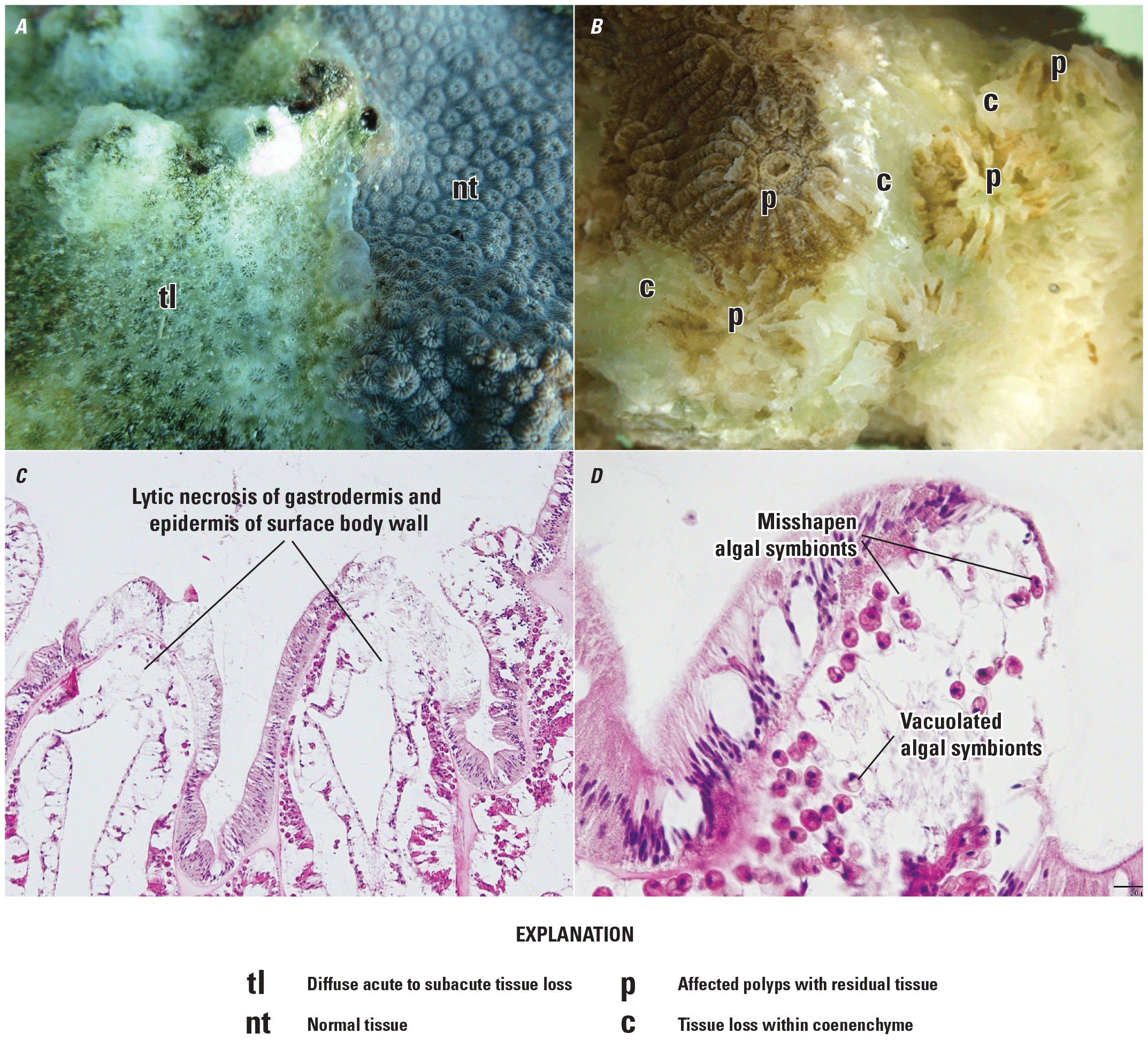
Orbicella faveolata gross, subgross and microscopic lesions. A, diffuse acute to subacute tissue loss with distinct to indistinct borders next to normal tissue (nt). Photograph by Vanessa Brinkhuis, Florida Fish and Wildlife Conservation Commission (FWC). B, subgross of affected polyps showing tissue loss in coenenchyme and fragments of residual tissues interspersed with intact bare skeleton. Photograph by Yasu Kiryu, FWC. C, lytic necrosis of gastrodermis and epidermis of surface body wall. D, lytic necrosis with misshapen and vacuolated algal symbionts endosymbionts. C and D are paraffin embedded hematoxalin and eosin photomicrographs by Jan Landsberg and Yasu Kiryu, FWC.
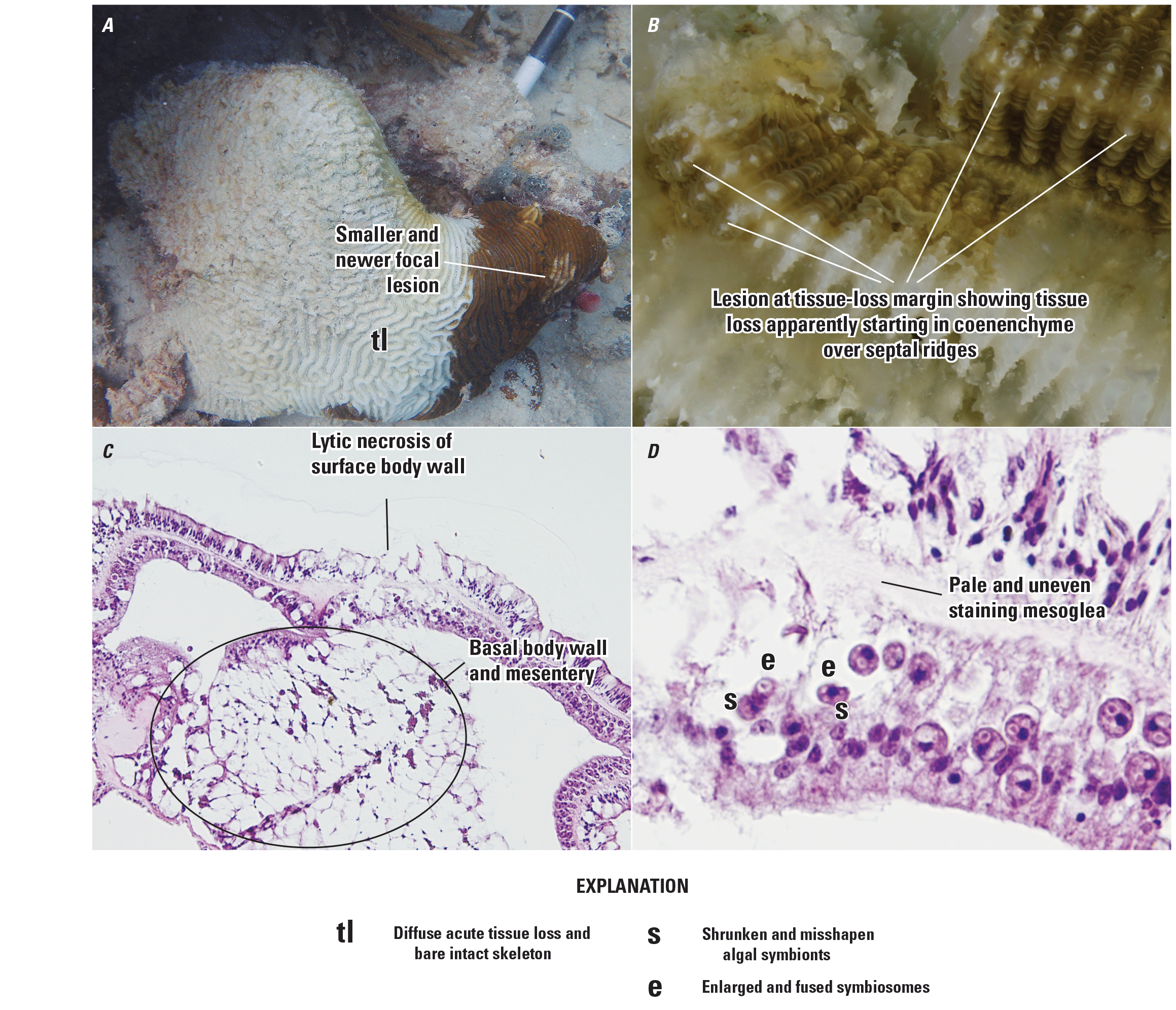
Pseudodiploria strigosa gross, subgross and microscopic lesions. A, diffuse acute tissue loss and bare intact skeleton with a smaller and newer focal lesion on the right. Photograph by Brian Reckinbeil, Florida Fish and Wildlife Conservation Commission (FWC). B, subgross image of lesion at tissue-loss margin showing tissue loss apparently starting in coenenchyme over septal ridges. Photograph by Jan Landsberg and Yasu Kiryu, FWC. C, lytic necrosis of gastrodermis of the basal body wall is expanded and distorted by severe vacuolations and lytic necrosis that extends entirely up one mesentery and into the body wall gastrodermis of surface body wall with disruption of the mesoglea and vacuolation of epidermis. D, affected algal symbionts are shrunken and misshapen with enlarged, fused symbiosomes and pale, uneven staining mesoglea. C and D are paraffin embedded hematoxalin and eosin photomicrographs by Jan Landsberg and Yasu Kiryu, FWC.
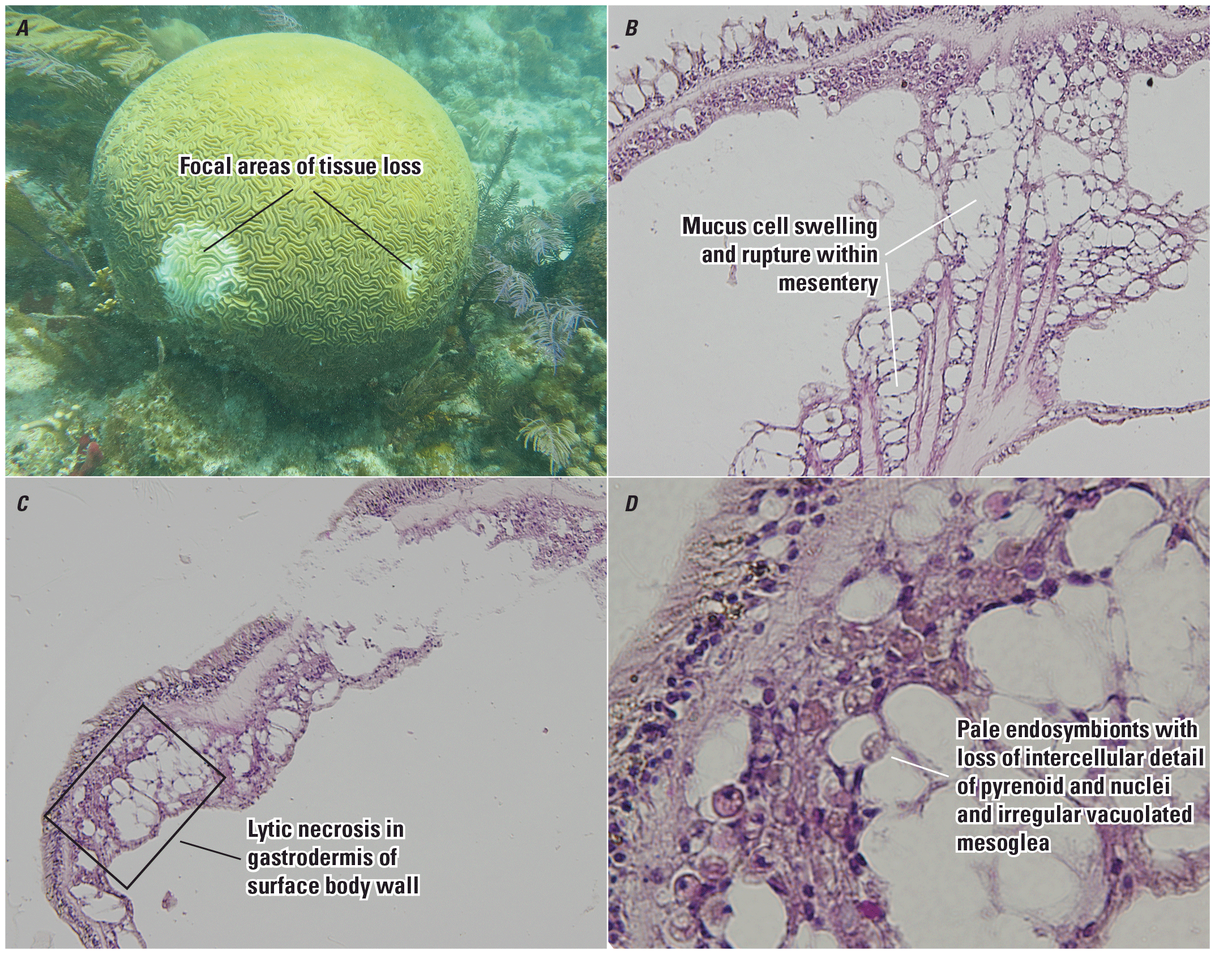
Diploria labyrinthiformis gross and microscopic lesions. A, focal areas of tissue loss. Photograph by Vanessa Brinkhuis, Florida Fish and Wildlife Conservation Commission (FWC). B, mucus cell swelling and rupture within gastrodermis of basal body wall and mesentery. C, lytic necrosis in gastrodermis of surface body wall. D, higher magnification of area defined by box in C showing pale endosymbionts with loss of intercellular detail of pyrenoid and nuclei and irregular, vacuolated mesoglea. B, C, and D are paraffin embedded hematoxalin and eosin photomicrographs by Jan Landsberg and Yasu Kiryu, FWC.
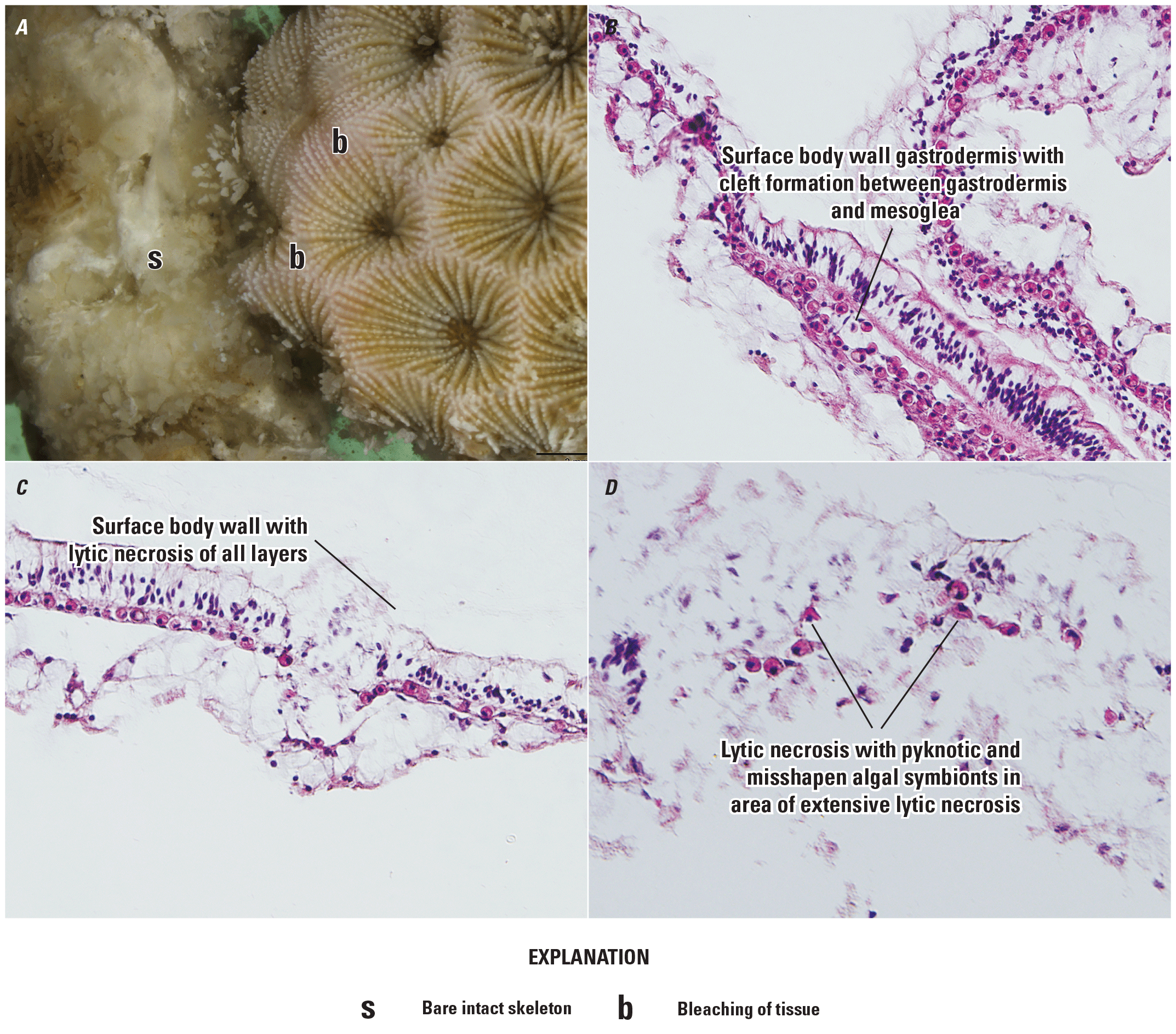
Siderastrea siderea subgross and microscopic lesions. A, subgross image of polyps at tissue loss margin showing bare skeleton and bleaching of tissue, as indicated by a pale lavender hue. Photograph by Yasu Kiryu, Florida Fish and Wildlife Conservation Commission (FWC). B, surface body wall gastrodermis with cleft formation between gastrodermis and mesoglea. C, surface body wall with lytic necrosis of all layers. D, lytic necrosis with pyknotic and misshapen algal symbionts in area of extensive lytic necrosis. B, C, and D are paraffin embedded hematoxalin and eosin photomicrographs by Jan Landsberg and Yasu Kiryu, FWC.
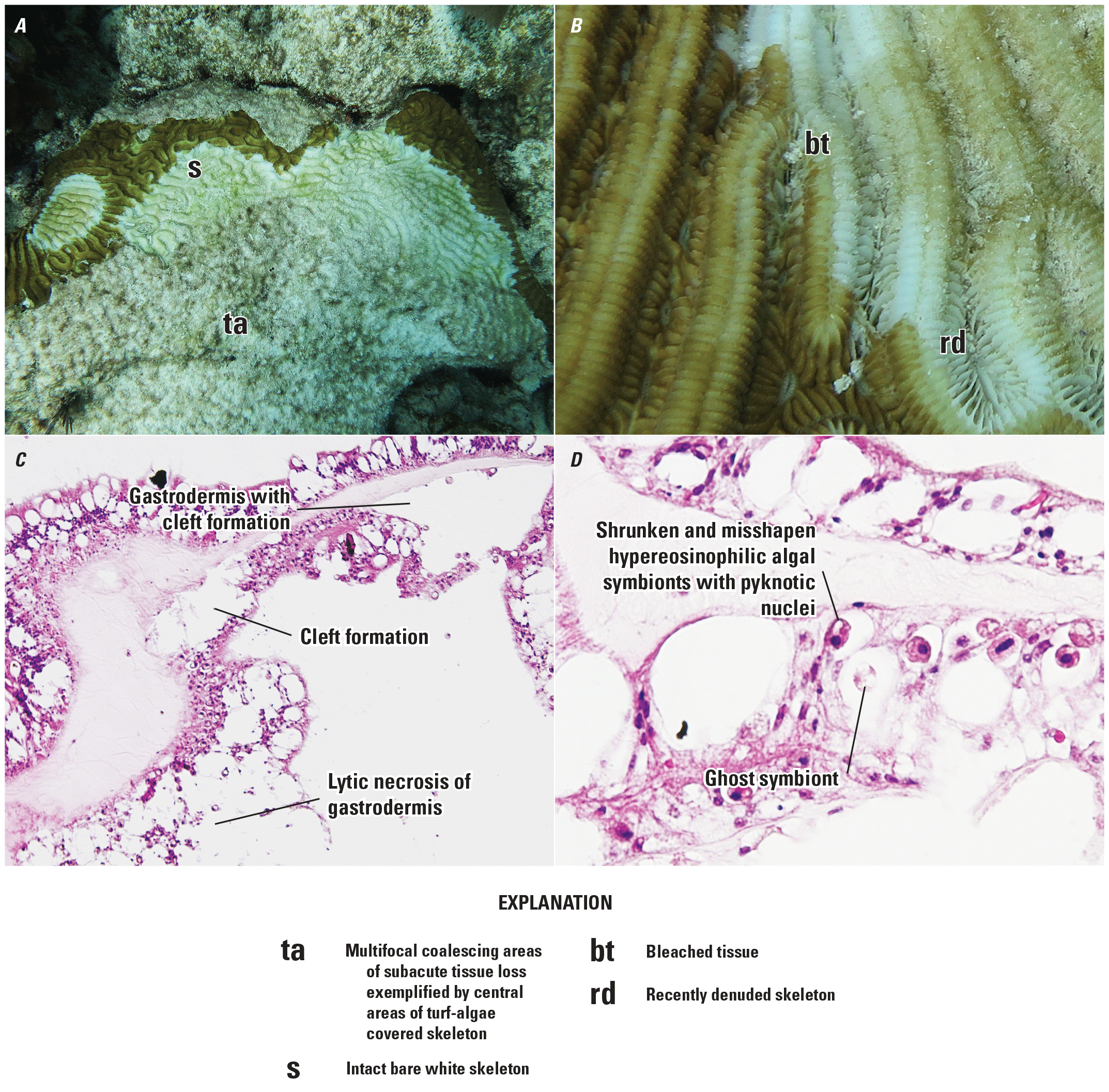
Colpophyllia natans gross and microscopic lesions. A, multifocal coalescing areas of subacute tissue loss exemplified by central areas of turf-algae covered skeleton separated from intact tissues by a band of intact white bare skeleton. Photograph by Vanessa Brinkhuis, Florida Fish and Wildlife Conservation Commission (FWC). B, subgross image of subacute lesion with white border indicating bleaching of tissue and recently denuded skeleton. Photograph by Vanessa Brinkhuis, FWC. C, gastrodermis with cleft formation and lytic necrosis. D, shrunken hypereosinophilic algal symbionts with pyknotic nuclei, ghost symbiont, and misshapen algal symbionts within enlarged symbiosomes. C and D are paraffin embedded hematoxalin and eosin photomicrographs by Jan Landsberg and Yasu Kiryu, FWC.
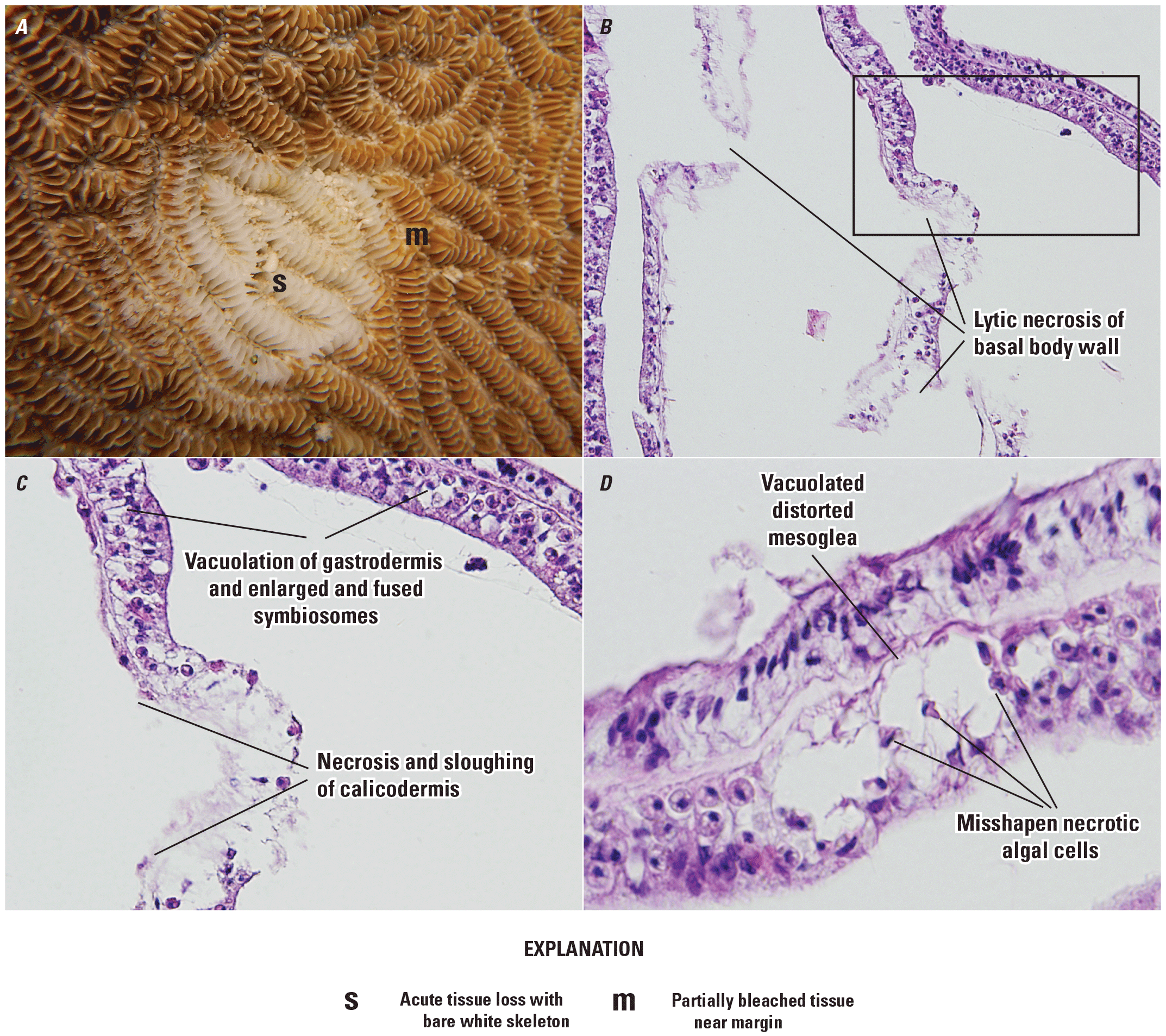
Meandrina meandrites subgross and microscopic lesions. A, acute tissue loss with bare, white skeleton bordered by intact and partially bleached tissue near margin. Photograph by Katie Cummings, Florida Fish and Wildlife Conservation Commission (FWC). B, lytic necrosis of basal body wall. C, magnification of box in B showing necrosis and sloughing of calicodermis, vacuolation of gastrodermis, and enlarged and fused symbiosomes. D, Misshapen, necrotic algal cells surrounded by vacuolated, distorted mesoglea. B, C, and D are paraffin embedded hematoxalin and eosin photomicrographs by Jan Landsberg and Yasu Kiryu, FWC.
In large-cup star coral and symmetrical brain coral, rhomboidal, 1- to 10-micrometer intracytoplasmic Periodic acid-Schiff (PAS)-positive and eosinophilic inclusions, or crystalline inclusion bodies (CIBs; presumably within the cytoplasm of mucocytes), have been seen in the basal body wall gastrodermis, sometimes within or at the periphery of lesions (including degenerating mucocytes); however, these are not always seen, and they may also be present in apparently healthy tissue (Landsberg and Kiryu, 2016; Landsberg and others, 2020). Basal body wall, calicodermis, and gastrodermal lesions are often present in the absence of surface or epidermal lesions, and mesoglea next to foci of necrosis is often disrupted or expanded with clear space (figs. 2F, 5D). Histologic lesions may be seen in coral from an affected reef that do not show gross signs of tissue loss.
Bacteria are not typically associated with lesions in hematoxylin and eosin-stained sections, but suspect bacteria in basal and surface body wall gastrodermis and cnidoglandular bands have been found using Giemsa, thionin, or Gram stains, some of which also bind to fluorophore-tagged eubacterial probes (EUB338-I, EUB338-II, EUB338-III) using onsite hybridization procedures (Esther Peters, George Mason Unversity, oral commun., 2020). Endolithic fungi or algae may be noted as are intracellular coccidia in the gastrodermis, but these are not a consistent feature, and their significance is uncertain.
Diagnostic test(s).—At present, the only diagnostic test to confirm SCTLD is light microscopy of paraffin embedded tissues stained with hematoxylin and eosin demonstrating the characteristic lesions described above.
Laboratory Criteria Categorization
Laboratory confirmed.—Gross and microscopic lesions demonstrating morphology described in the “Laboratory Criteria for Diagnosis” section.
Laboratory supportive.—Gross lesions compatible with SCTLD in a susceptible species, including high suspicion if other susceptible species on the same reef are also affected.
Exposed.—Not applicable.
Present/detected.—Not applicable.
Epidemiologic Linkage Criteria for Diagnosis
An epidemiologic linkage can be established by close geographic and temporal proximity (in other words, part of the same mortality event) as one or more confirmed cases of SCTLD or at a site with a recent history of confirmed SCTLD with similar presentation as described in the “Case Definition Criteria” sections.
Case Classification
The sum of the criteria listed in the “Case Definition Criteria” sections (individual, place, time, field, laboratory, and epidemiologic linkage criteria) associated with a particular disease or pathogen/toxin in an individual animal or specimen add up to a case classification (fig. 10; table 1).

Case definition criteria add up to the case classifications. From Miller and others (2024).
Depending on the confidence in the results, cases of a specific disease will be classified as “confirmed,” “presumptive,” or “suspected;” and evidence of a pathogen or toxin will be classified as “exposed” or “present/detected” (table 1; refer to glossary for definitions). A specific case classification may have more than one pathway to it. Not all classifications may be used for every disease. Although an epidemiological linkage may be present in all classifications, the “suspected” case classification requires compatible epidemiological linkage criteria are met. Individual disease and pathogen specific details are presented in table 1.
Note.—The field and laboratory criteria in table 1 reflect the typical presentation of SCTLD. The exact presentation in an individual animal or specimen may vary from what is presented in table 1 but should still conform with the information presented in the “Field Criteria for Diagnosis” and “Laboratory Criteria for Diagnosis” sections.
Table 1.
Case classification chart for stony coral tissue loss disease.[The suspected, exposed, and present/detected case classifications do not apply to this case definition]
Quality Assurance Review Schedule
The authors plan to review this case definition periodically to incorporate new scientific information and test methods as needed.
Planned date for next review.—June 1, 2025
Schedule.—June 2025 and then every 3–5 years—or sooner if science about SCTLD changes substantially.
Impact
Applying case definitions in diagnostic, surveillance, and research efforts can help standardize data, making it easier to understand and analyze within and between diagnosticians and laboratories. Laboratories are encouraged to store the case classification assigned to each specimen or sample in their data system so that it can be readily and reliably retrievable.
References Cited
Aeby, G.S., Ushijima, B., Campbell, J.E., Jones, S., Williams, G.J., Meyer, J.L., Häse, C., and Paul, V.J., 2019, Pathogenesis of a tissue loss disease affecting multiple species of corals along the Florida Reef Tract: Frontiers in Marine Science, v. 6, 18 p. [Also available at https://doi.org/10.3389/fmars.2019.00678.]
Alvarez-Filip, L., Estrada-Salvidar, N., Perez-Cervantes, E., Molina-Hernandez, A., and Gonzalez-Barrios, F.J., 2019, A rapid spread of the stony coral tissue loss disease outbreak in the Mexican Caribbean: PeerJ, v. 7, e8096. [Also available at https://doi.org/10.7717/peerj.8069.]
FDEP, 2018, Case definition—Stony Coral Tissue Loss Disease (SCTLD): Florida Disease and Epidemiology Team, accessed August 5, 2020, at https://floridadep.gov/rcp/coral/documents/stony-coral-tissue-loss-disease-sctld-case-definition.
Landsberg, J.H., and Kiryu, Y., 2016, 2016 coral disease epizootic (update II): Florida Fish and Wildlife Conservation Commission, accessed August 2020 at https://floridadep.gov/rcp/rcp/documents/2016-coral-disease-epizootic.
Landsberg, J.H., Kiryu, Y., Peters, E.C., Wilson, P.W., Perry, N., Waters, Y., Maxwell, K.E., Huebner, L.K., and Work, T.M., 2020, Stony coral tissue loss disease in Florida is associated with disruption of host–zooxanthellae physiology: Frontiers in Marine Science, v. 7, no. 1090, 24 p. [Also available at https://doi.org/10.3389/fmars.2020.576013.]
Marks, K.W., and Lang, J.C., 2018, AGARRA database and summary products (ver. 2018-03): Atlantic and Gulf Rapid Reef Assessment digital data, accessed December 2020 at http://www.agrra.org/data-explorer/explore-summary-products/.
Meiling, S., Muller, E.M., Smith, T.B., and Brandt, M.E., 2020, 3D photogrammetry reveals dynamics of stony coral tissue loss disease (SCTLD) lesion progression across a thermal stress event: Frontiers in Marine Science, v. 7, 12 p. [Also available at https://doi.org/10.3389/fmars.2020.597643.]
Meiling, S.S., Muller, E.M., Lasseigne, D., Rossin, A., Veglia, A.J., MacKnight, N., Dimos, B., Huntley, N., Correa, A.M.S., Smith, T.B., Holstein, D.M., Mydlarz, L.D., Apprill, A., and Brandt, M.E., 2021, Variable species responses to experimental stony coral tissue loss disease (SCTLD) exposure: Frontiers in Marine Science, v. 8, no. 464, 12 p. [Also available at https://doi.org/10.3389/fmars.2021.670829.]
Miller, M.W., Karazsia, J., Groves, C.E., Griffin, S., Moore, T., Wilber, P., and Gregg, K., 2016, Detecting sedimentation impacts to coral reefs resulting from dredging the Port of Miami, Florida USA: PeerJ, v. 4, p. e2711. [Also available at https://doi.org/10.7717/peerj.2711.]
Miller, K.J.G., Parmley, E.J., Ballmann, A., Buckner, J., Jones, M., Lankton, J.S., Zimmer, M., and Lankau, E., 2024, [Disease/condition] case definition [template] for wildlife: U.S. Geological Survey Techniques and Methods, book 19, chap. A1, 8 p., https://doi.org/10.3133/tm19A1.
Muller, E.M., Sartor, C., Alcaraz, N.I., and van Woesik, R., 2020, Spatial epidemiology of the stony-coral-tissue-loss disease in Florida: Frontiers in Marine Science, v. 7, 11 p. [Also available at https://doi.org/10.3389/fmars.2020.00163.]
Precht, W.F., Gintert, B.E., Robbart, M.L., Fura, R., and Van Woesik, R., 2016, Unprecedented disease-related coral mortality in southeastern Florida: Scientific Reports, v. 6, no. 1, 11 p. [Also available at https://doi.org/10.1038/srep31374.]
Sharp, W., and Maxwell, K., 2018, Investigating the ongoing coral disease outbreak in the Florida Keys—Collecting corals to diagnose the etiological agent(s) and establishing sentinel sites to monitor transmission rates and the spatial progression of the disease: Florida Fish and Wildlife Conservation Commission, 26 p.
Work, T.M., and Aeby, G.S., 2006, Systematically describing gross lesions in corals: Diseases of Aquatic Organisms, v. 70, p. 155–160. [Also available at https://www.int-res.com/articles/dao2006/70/d070p155.pdf.]
Work, T.M., Weatherby, T.M., Landsberg, J.H., Kiryu, Y., Cook, S.M., and Peters, E.C., 2021, Viral-like particles are associated with endosymbiont pathology in Florida corals affected by stony coral tissue loss disease: Frontiers in Marine Science, v. 8, 18 p. [Also available at https://doi.org/10.3389/fmars.2021.750658.]
Glossary
additional diagnostic comments
Any additional diagnostic notes pertinent to recording/reporting (for example, requests for strain/serovar/variant reporting, inconclusive/ambiguous results, or “not applicable”).
case classification
The sum of the factors in the “Case Definition Criteria” sections of the case definition including individual (for example, species, age group), place, time, history, clinical signs, diagnostic observations, and (or) diagnostic test results, associated with a particular disease or pathogen/toxin in an individual animal or specimen. Depending on the confidence in the results, cases of a specific disease will be classified as “confirmed,” “presumptive,” or “suspected;” and a pathogen or toxin will be classified as “exposed” or “present/detected.”
case definition
A consistently applied, scientifically based and clearly defined set of field, gross, histopathology, laboratory, or epidemiologic criteria used to classify an individual animal or sample to a specific disease or pathogen/toxin for surveillance or outbreak reporting purposes (based on the combination of the criteria and confidence in the results).
confirmed case
The combination of individual (for example, species, age group), place, time, history, clinical signs, and laboratory criteria for diagnosis with the highest level of certainty for accepted diagnostic testing as stated in the case definition. Example: Cardinal with clinical signs, gross and microscopic lesions compatible with salmonellosis, and positive bacterial culture for Salmonella enterica enterica in the liver.
diagnostic test(s)
Laboratory tests typically used to determine this diagnosis or detect the pathogen/toxin; for example, bacterial culture.
diagnostically compatible
An animal that meets the individual (for example, species, age group), place, time, field, and laboratory criteria for a particular disease as stated in the case definition.
disease
Any disorder of structure or function that may produce specific clinical signs; disease can be infectious or noninfectious.
disease agent
Any pathogen, toxin, or other known cause of disease.
epidemiologically linked
A case that has temporal, geographic, or other relevant linkages to one or more confirmed cases as described under “Epidemiologic Linkage Criteria for Diagnosis” in the case definition.
exposed
Detection of a toxin in tissues or body fluids at a concentration above acceptable background levels but below the documented lethal threshold level for the species. This may apply to a toxin detected in the absence of documented lethal threshold levels. This category can also include serological evidence of infection in the absence of other information such as organism detection or disease diagnosis.
gross examination
Gross necropsy observations in a carcass or sample that are diagnostically compatible with disease.
histopathology
General microscopic observations in a carcass or sample that are diagnostically compatible with disease.
history and clinical signs
Field observations and changes in behavior, appearance, or abilities in live animals/populations that are diagnostically compatible with disease. Photograph or video evidence may be used when appropriate.
individual
The common age groups, species, or other characteristics that increase disease or pathogen/toxin suspicion.
laboratory confirmed
The strongest degree of assurance in identification of a disease agent of interest and evidence of the associated disease based on one or more accepted laboratory methods. A test or combination of methods that has been scientifically accepted as definitive for a particular disease agent and the associated disease. Example: Positive bacterial isolation for salmonella plus compatible gross and histologic lesions for salmonellosis.
laboratory criteria for diagnosis
The gross, microscopic, molecular, culture, analytical or other laboratory test criteria used to determine the presence of a specific disease agent and evidence of the disease itself. These are categorized based on the validity and performance of the test(s). Categories are “laboratory confirmed,” “laboratory supportive,” “exposed,” and “present/detected.” Where possible, references for the current accepted science for a given disease and pathogen are provided in the case definition. For some select new or emerging diseases the laboratory criteria may be based on the collective expertise of pathologists at the U.S. Geological Survey National Wildlife Health Center and the Canadian Wildlife Disease Cooperative or other institutions.
laboratory supportive
Laboratory results that are less than definitive for a specific disease agent and the associated disease. A test or combination or methods whose results support the diagnosis or a particular disease but are not considered definitive; for example, a screening test. Test result interpretation may be based on the tissue tested (for example, culture of amphibian skin surface versus internal tissue) or postmortem condition of the sample. Example: Gross and histologic lesions compatible with salmonellosis (without laboratory testing).
notifiable/reportable disease
A disease or pathogen that by law must be disclosed to State, Provincial, and (or) Federal agricultural or public health authorities.
other (field criteria)
Additional pertinent comments about presentation (for example, potential for carrier status).
place
Locations and other geographic features that increase disease or pathogen/toxin suspicion.
present/detected
Laboratory detection of a potentially pathogenic agent in the absence of findings diagnostically compatible with the associated disease. Often used when tracking a known or suspected asymptomatic carrier state (for example, Salmonella or duck virus enteritis) or when documenting detection of an agent that is of increased diagnostic or epidemiologic interest, even in the absence of evidence of illness (for example, new or emerging disease or syndrome).
presumptive case
The combination of individual (for example, species, age group), place, time, history, clinical signs and laboratory criteria for diagnosis that has a moderate degree of certainty as stated in the case definition. This uncertainty may be due to the test performed, postmortem decomposition of the carcass affecting observation or interpretation of gross and or histopathologic lesions, inadequate sample for testing due to scavenging or carcass size, inconclusive test results, or lack of a definitive diagnostic test. Enough information is available to conclude the disease is most likely present but not enough information available to conclude the disease is definitively present. Example: Raccoon with compatible histologic lesions for parvovirus without additional laboratory test results.
scope
Indicates what species, when and (or) where this protocol applies; for example, specifics regarding the disease agent, animal class, sex, age group, location, season, antemortem or postmortem sample collection, environmental samples, and so on.
suspected case
This is primarily based on a combination of individual, place, time, minimal or nonspecific field and laboratory information and a geographic and temporal (epidemiologic) connection to a confirmed case. Not enough information is available to meet the threshold in the case definition for a confirmed or presumptive case, but the diagnosis can reasonably be inferred by the close association with confirmed cases of a particular disease in other animals collected from the same general location and time. Example: A specimen with a geographic or temporal link to a confirmed case of a disease that is not tested but was examined and may have nonspecific gross or histopathologic findings that are compatible with that disease.
time
The season(s), months, or other temporal factors that increase disease or pathogen/toxin suspicion.
wildlife
Free ranging vertebrate species (mammals, birds, reptiles, amphibians, and fish).
For more information about this publication, contact:
Director, USGS National Wildlife Health Center
6006 Schroeder Road
Madison, WI 53711
For additional information, visit: https://www.usgs.gov/centers/nwhc
Publishing support provided by the Rolla Publishing Service Center
Disclaimers
Any use of trade, firm, or product names is for descriptive purposes only and does not imply endorsement by the U.S. Government.
Although this information product, for the most part, is in the public domain, it also may contain copyrighted materials as noted in the text. Permission to reproduce copyrighted items must be secured from the copyright owner.
Suggested Citation
Hawthorn, A.C., Dennis, M., Kiryu, Y., Landsberg, J., Peters, E., and Work, T., 2024, Stony coral tissue loss disease (SCTLD) case definition for wildlife: U.S. Geological Survey Techniques and Methods, book 19, chap. I1, 20 p., https://doi.org/10.3133/tm19I1.
ISSN: 2328-7055 (online)
Study Area
| Publication type | Report |
|---|---|
| Publication Subtype | USGS Numbered Series |
| Title | Stony coral tissue loss disease (SCTLD) case definition for wildlife |
| Series title | Techniques and Methods |
| Series number | 19-I1 |
| DOI | 10.3133/tm19I1 |
| Publication Date | April 11, 2024 |
| Year Published | 2024 |
| Language | English |
| Publisher | U.S. Geological Survey |
| Publisher location | Reston, VA |
| Contributing office(s) | National Wildlife Health Center |
| Description | v, 20 p. |
| Country | United States |
| State | Florida |
| Other Geospatial | Dry Tortugas, Florida Reef Tract |
| Online Only (Y/N) | Y |
| Additional Online Files (Y/N) | N |